Spent considerable time debating whether or not to include the story in the blog but it has had a tremendous impact on my life (the Missus’ too) and influenced cycling goals and aspirations. Besides, my blog, my rules. So, it was the 2019 racing season and I was competing in the local USA Cycling Time Trial series. There was supposed to be a total of 6 races over 5 different courses ranging between 28K and 31 miles in the series. Extremely familiar with one of the courses but others were unknown. The plan was to ride each course prior to the actual event as route familiarization lessens the mental anxiety associated with the race. Well, successful recon performed at all sites, even the route that was subsequently canceled, except for one. Correct. Except for the one that led to the guardrail incident. Did review the RideWithGPS file and knew there was a descent around the 5-mile mark but nothing else noteworthy in the file. What could go wrong, right? Answer is – a lot!
Sure enough, descent started around 4.5- mile mark and picked up quite a bit of speed. Too much speed. Near the bottom of the descent was a sweeping curve to the left. TT rim brakes aren’t known for their stopping power and unable to successfully navigate the turn. Rode the guardrail for a bit then, crash! Next I knew I was laying on my back, in the wood line, on the other side of the guardrail. A cursory inventory of the damage revealed a clean, nearly 5-inch long laceration on the inside of my right forearm. The flap of skin was laid back, exposing all the things one isn’t supposed to see – tendons, ligaments, radial artery. Also had a puncture wound in upper arm apparently caused by impaling myself on 1-inch diameter stick. Never lost consciousness and thankfully didn’t have to wait too long before a course official discovered me and called 911. Mildly uncomfortable getting strapped to the backboard when the EMS team arrived. Experienced a new pain in the right leg when feet were positioned to allow straps to be tightened. Annoyingly, had to keep repeating my name and the Missus’ contact number while the EMS made several attempts to contact her and let her know where they were taking me. The Missus was out for her run and she had a few, nonspecific voice mails waiting for her upon her return to the house. Meanwhile, I’m off to the largest full-service hospital in the area.
The initial shock soon wore off and discomfort levels increased until an IV was inserted and goodness started flowing. To be honest, don’t recall all of the activities upon reaching the hospital, relocating to gurneys, x-rays, and other triage actions. While the forearm wound was being stitched close, learned my leg was broken. Didn’t pay too much attention until one of the nurses indicated I was being admitted for an overnight stay. Turns out it was not just any break but a tibial plateau fracture (TPF). There would be no cast. Scheduled for surgery the following morning to have an external fixator (Ex-Fix) applied/installed/attached. At some point The Missus, girl child and fiancée made it to the hospital. The Missus was a wreck and devastated to see me lying in bed with my forearm and leg all wrapped up.
A TPF is a break or fracture in the top of the shin bone and are graded on a 1-6 score. Ever the high achiever, mine was a grade 6 but non-displaced. Additionally, there was no damage to tendons, ligaments, muscles, meniscus, or skin. The only visible sign was a small mark just below the knee – the impact site of the guardrail. While there wasn’t any collateral damage, there was still significant trauma to the area. The Ex-Fix is used to allow the body to begin recovering from the trauma, naturally clear out the impact site, and most importantly, reduce the risk of infection following the actual procedure to fix the break. My Ex-Fix consisted of 2 bolts attached to the outside of my femur and 2 bolts attached to the inside of the tibia. Two titanium rods connected the bolts keeping the bones properly aligned. The 4 bolts protruded about 2.5 inches through the skin. A little gruesome thinking about, slightly nauseating looking at it, and rather painful feeling it. Extremely fortunate to have an excellent orthopedic surgeon on staff. The Missus would be driving me 2+ hours one way for every follow-up visit. Pain was intense but nothing a combination of dilaudid and oxy couldn’t handle although only had the former for the first 24 hours. Bad nights’ sleep were just beginning. Discharged from the hospital after a two day stay. Mobility was a learning process and would make friends with a walker. Sat in the back seat, sideways, for the drive home. That was not a comfortable trip. The Ex-Fix would be part of me for the next 16 days and only the beginning of the non-weight bearing time. As the head of the bone isn’t as hard as the shaft, any load placed on a TPF risks worsening the fracture or causing a displacement of a bone fragment. Then things really get ugly.








Good to be home. Neighbors helped the Missus bring two of the recliners from downstairs up to the living room where I would spend most of the next two weeks. What followed was not an experience I would wish on anyone. Truly miserable and not even possible without the assistance of the Missus. Thankfully, had both short- and long-term disability insurance through my employer so didn’t have financial considerations hanging over my head. Spent most of my days on my butt reading (sci-fi/fantasy) but not much tv viewing. The Missus stayed home from work a lot to provide care and company. The skin around the ex-fix bolts had to be cleaned every day and new gauze applied. Showering wasn’t an option so wash cloth or shower wipes with an occasional hair washing in the kitchen sink. I could relocate from the living room to the bedroom with a walker but that was about the extent of it. Bathroom activity wasn’t enjoyable. Had a portable, collapsible commode and urinal bottle. Using bathroom toilet was a little too strenuous as it sits much closer to the floor compared to the portable unit. One legged squats were never a favorite and adding the extra weight and anxiety of the Ex-fix didn’t improve the odds of successful execution. Sleep was another issue. Diagnosed with Obstructive Sleep Apnea (OSA) in 2011 and prescribed a CPAP machine for treatment. Behavioral modifications were ironic and laughable – stop smoking (don’t), lose weight (good one), exercise more (you’re kidding, right?), reduce alcohol consumption (then what would I do with my wine cellar and Hopsy?), position therapy (sleep on your side; umm, I have this contraption screwed into my leg the kinda makes that impossible). The CPAP machine exacerbated my Periodic Limb Movement Disorder and Restless Leg Syndrome. End result: OSA treated but still not sleeping. Once asleep, movement disorders usually weren’t sufficient to cause wakening. However, waking up within 90 minutes or so of falling asleep created problems and kicked the movement maladies into high gear. The only way to stop the unwanted activity is to stand for 10-15. Unfortunately, that remedy was no longer an option. Oh, the pain also would ratchet up at night. Sometimes the oxy was effective, other times, not so much. Welcome to my nightmare. Daytime napping wasn’t an option as that would further contribute to the nighttime sleep dilemma. Normally PLMD and RLS restrict their impact to the sleeping hours but since my activity was basically zero, they decided to make it an all-day affair. Having your leg twitch and spasm uncontrollably while titanium rods are attached to bolts drilled into your bones for the express purpose of keeping the leg properly aligned is not a pleasant experience. Enjoyed several all-night twitch fests with the Ex-Fix. The Missus was nice enough to sacrifice her night’s sleep so we could both watch my legs do the horizontal dance.
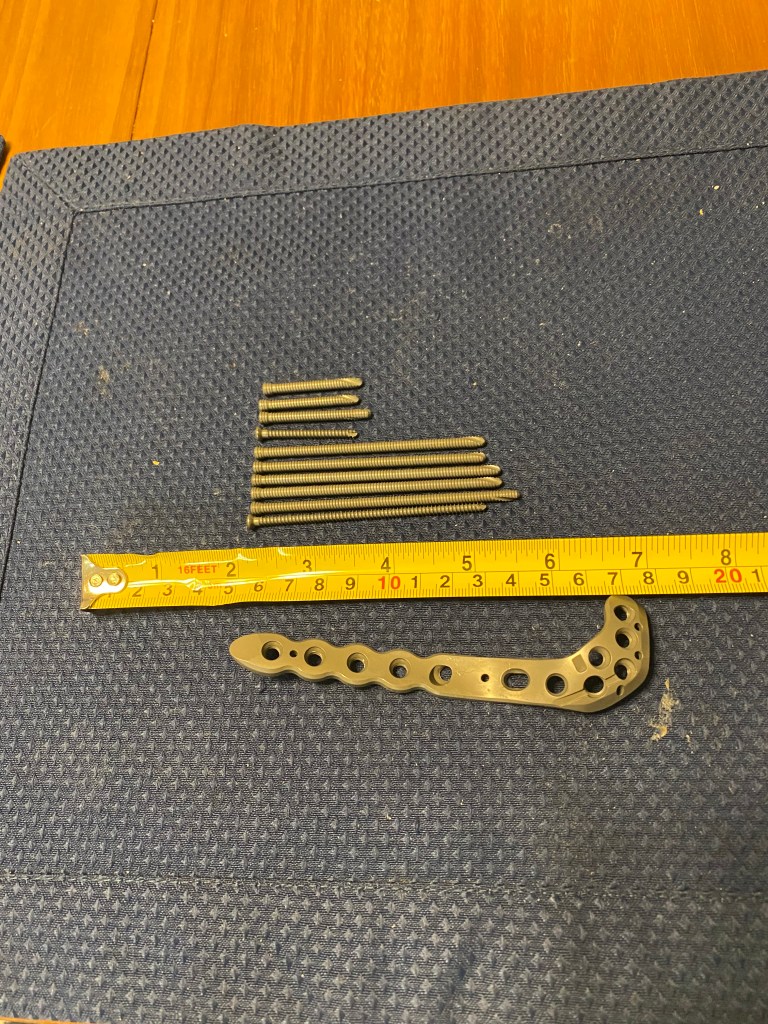
Finally, the day came for the corrective procedure – plate and screws (referred to as the dragon tail) inserted to keep the tibial head together so it could heal. Early morning procedure meant making the 2+ hour drive the day before and staying at a nearby Hampton Inn. Have stayed at dozens of locations across the county and usually have an uneventful experience. Well, must’ve been some local event because the hotel was full and loud. Elevators were barely big enough to accommodate a wheelchair. The procedure was supposed to be an out-patient one with hospital discharge occurring on the same day. Well, body didn’t respond well. Blood pressure remained low and on the short shuffle to in-room bathroom, nearly passed out on the toilet. Check-out was delayed a day and the Missus stayed with me the entire time. Although she was able to secure a room for herself the second night as she didn’t get much sleep staying in my room – nighttime medicine deliveries, recording of vital signs and the monitors repeatedly going off because it didn’t like it when my heart rate dropped below 42 bpm; a very common occurrence during sleep. Successfully passed the blood pressure test, maneuvered to the restroom, and shuffled around with the aid of a walker. Also had a brief tutorial in the use of crutches as now the non-weight bearing clock could actually start: 90 days and counting.





Leg was all wrapped up in a knee immobilizer so still had to sit in the back seat for the drive home. Had to keep the knee immobilizer on for one week. Returned to my normal position in the living room recliner. Far more mobile without the Ex-Fix but recommend staying off one leg (you can even pick which one) for a couple of days. Amazing how tiring it gets only standing on one leg. Post procedure pain wasn’t nearly as bad as after the Ex-Fix but wasn’t a picnic either. Sleeping still wasn’t much better. A week eventually passed and able to remove the knee immobilizer and begin range of motion (ROM) exercises. Simply astounding at the loss of flexibility after just over 3 weeks of not bending the knee. Normal knee ROM range is 0-135° while functional ROM (amount of movement needed for daily tasks) is 120°. Don’t know starting point but left leg flexion was 155° and extension was 185° My guess is active right knee ROM (unassisted) was 45° and active assisted (muscle contraction and pulling heel towards buttocks) was certainly less than 90°. Such a long way to go.

Spent a fair bit of time over the next 3 weeks in the recliner and sitting on the floor doing active assisted exercises to increase range of motion along with dorsi/plantar flexion of the ankle. Ten days post-surgery made another 2+ hour trip for a follow up and removal of stitches. Had increased active ROM to a little more than 90°. Beginning the 4th week following surgery, had a physical therapist come to the house 2-3 days/week to work on ROM, strength and perform lymphatic massage. One of the other side effects to the initial trauma and subsequent Ex-Fix and corrective surgery is swelling in the ankle and foot. However, in my case it was ankles and feet. Even the non-injured leg experienced the symptoms. Thankfully, I was allowed to get back on the bike – trainer, only. The therapist thought I was crazy when walker-shuffled out to the garage and climbed onto the saddle. Used a modified triathlon transition approach to clip into the pedals: slipped the left shoe on my foot but had the right shoe already clipped in. Secured the left shoe then swung the right leg of the saddle to rest gently on the shoe. Slowly and gently eased the foot into the shoe and off to the races. Not quite. Started with a single 5-minute session and gradually increased to two 15-minutes daily (morning and afternoon) sessions over the next six weeks. To ensure minimal resistance while pedaling, the chain was removed. Now that will force concentration on a smooth pedal stroke. Over that same time period, reached 154° of passive knee flexion (full range of motion), 135° of active knee flexion (still a work in progress), and full ROM at the ankle. It wasn’t easy, required daily work, there were tears.





The next follow-up was 9 weeks after surgery. X-rays revealed the bone was healing but cracks were still visible. Asked the Doc if the chain could be back on the bike. His response, “I don’t care what you do on the bike.” The Missus’ response was classic. Her eyes got real big, she stood up, and forcefully said, “You don’t know what that means to him.” It was humorous to watch the Doc backpedal (no pun intended) on his statement. He revised his comment to, “Well, you could do what I would do on the bike.” Which I promptly responded, “I don’t know what that means.” We kind of came to an agreement that I wouldn’t get crazy, but he still had no idea. Made promises to the Missus that progress would be slow and steady. Progress was steady, maybe not slow but ramped from 30’ to 60’ over the next week then started Zwift “D” rides.
The 12-week post-surgery date finally arrived and weight bearing was allowed. Learning to walk again. Tend to take advantage of the little things. Girl Child, a physical therapist, and the Missus offered support and encouragement as the first steps in nearly 3 ½ months were taken; with the assistance of a collapsible cane (more on that shortly). Thinking about all of the actions necessary for a regular gait was a little overwhelming at first: knee lift, extend, heel strike, toe off. Didn’t limp too badly but couldn’t be helped. A little discomfort and loss of strength not to mention the incredibly shrinking thigh circumference – about a two inch girth difference between left and right.
First outdoor ride was 12 weeks and one day following plate and screw surgery. A teammate and friend agreed to chaperone since the Missus wasn’t too keen and the first outdoor ride being solo. Riding was easier than walking but hard to do one without the other. Solution was a collapsible cane broken down and placed in one of the jersey back pockets. The conundrum with cycle was which foot to keep clipped. Normally I keep the left foot clipped when coming to a full stop. Maintaining this routine meant clipping in and out, leaning to the right and then balancing on right foot at stops, and then a slight push-off with recovering leg to get started again. Tried both ways and wasn’t very comfortable either way. Ended up staying with previous routine – just very gently and slowly coming to a stop.
Completed a small group 70-miler (detour forced and extra 10 miles) withing two weeks of the first outside ride then it was no turning back. FTP was 90% of pre-crash number four weeks later. Have yet to reach previous mark (4.1 w/kg) but training focused shifted as COVID-19 pandemic arrived a few months later. Not sure I’ll compete in road races any more but still have TT goals.
Gravel is now a part of the training. A little before gravel riding started, began to experience knee and lower leg discomfort. There was never a time I couldn’t focus on the leg and feel the plate. Then walking started aggravating the leg with a return to ankle and foot swelling. Although it was never a consideration after the surgery, the orthopedic surgeon said everything could be removed after a year if it became a bother.
Well, 26 months after the corrective procedure with plate and screws, everything came out. Slicing the nicely healed scar back open, a local orthopedic trauma surgeon performed the out-patient procedure. It was quite the hardware selection. Rather shocking actually. Took a few days off, more than initially planned as the level of discomfort was greater than anticipated. Brought back a lot of memories – most of them unfavorable. At least weight bearing activity was permitted immediately although did use a single crutch for a couple of days. No running (sadly stopped that due to other reasons), swimming (not since the last sprint triathlon in 2017), or plyometrics for a few weeks. Didn’t miss the feet swelling and likely increased the leg strength/girth/balance disparity that still remain two years after the guardrail incident. Back on the trainer 3 days afterwards and promised the Missus I would remain indoors for the next two weeks. Finally paroled to outdoor riding just in time for the final organized ride of the season, The Great Pumpkin Ride. It’s the only organized ride that I stop at every rest stop. Because, each stop is full of pumpkin flavored goodies. Unfortunately, COVID-19 made a continued unwanted presence by significantly reducing the quantity and variety of mileage bonus snacks. Not complaining, too much, because they were all good. October was intended to be the recovery month and it continues to be but looking forward to new cycling adventures in 2022. Will give randonneuring a try – 1200K (non race, largely unsupported) over 4 consecutive days. Why not? And another Bicycling Adventures tour – WYMODAK, a ten-day trek across Wyoming, Montana, and South Dakota.